Myths, madness and insane ears
Published in Features, Issue 2 (March/April 2017), Volume 25Making sense of the history of psychiatry in Ireland
By Brendan Kelly

Above: Cathaoir Ana (Madman’s Chair) at Dunany Point, Co. Louth, was said to attract the mentally ill, who sat on it three times to be cured. Those who were not mentally ill and sat on it might become mad. According to another account, if a mad person sat on the rock during a period of lucidity, that lucidity would be maintained for life.
Early Irish literature and folklore are replete with references to madness. Stories such as the Táin Bó Cúalnge (‘The Cattle Raid of Cooley’), the central epic of the Ulster cycle, present vivid descriptions of altered states of mind. The arrival of Christianity saw the emergence of beliefs that insanity was attributable to possession by the devil or punishment by God, and the phrase duine le Dia (‘person of God’) came into use for persons with intellectual disability.
One story tells how a Norman archer became mad after entering the sacred area surrounding a perpetually burning fire lit by St Brigid in Kildare. This man blew on the fire and became insane, blowing into people’s mouths and running from house to house blowing on every fire he could find. He was seized by his comrades and, at his request, brought to water where, thirsty from all the blowing, he drank so much that he burst and died on the spot.
But it is the story of Suibhne Geilt (Mad Sweeney) that reveals the true fate of the mentally ill in pre-asylum Ireland. This epic tale was written in the twelfth century but has origins in the ninth century or earlier. The story is a vivid one, brilliantly reimagined in comic form by Flann O’Brien in At Swim Two Birds (1939) and magically retold by Seamus Heaney in Sweeney astray (2001). Sweeney, a chieftain, was cursed by Ronan the Fair, abbot of Drumiskin, and condemned to a life of madness, flying and wandering through the world.
Maddened by the slaughter at the battle of Moyrath in 637, Sweeney duly flew into the air from the battlefield and in this altered state turned away from mankind to live with the birds and animals in the wilderness. For many years he wandered from tree to tree (commonly the yew), having strange, disturbing visions. In the end, he joined a community linked with St Moling but was speared to death by a swineherd who wrongly accused him of adultery with his kindly, charitable wife. In all of its torment, tragedy and isolation, Sweeney’s story reflected not only contemporary views of the loneliness of madness but also tensions between pre-Christian and Christian Ireland, demonstrated vividly in Sweeney’s unresolved disturbance and dislocation.
‘Of all human calamity, I know of none equal to this’
Sweeney’s tale also reflected the lived experience of the mentally ill in Ireland up to the early 1800s. Most endured lives of destitution and early death, despite the establishment of St Patrick’s Hospital in Dublin in 1746, thanks to a bequest from Jonathan Swift, and two further asylums (one private, one public) by Dr William Saunders Hallaran in Cork in the 1790s.
In 1817 Robert Peel, the chief secretary, prevailed upon the House of Commons of the United Kingdom of Great Britain and Ireland to set up a select committee to look into the plight of ‘the lunatic poor in Ireland’. The Right Honourable Denis Browne (MP for Mayo) gave evidence:
‘There is nothing so shocking as madness in the cabin of the peasant, where the man is out labouring in the fields for his bread, and the care of the woman of the house is scarcely sufficient for the attendance on the children. When a strong young man or woman gets the complaint, the only way they have to manage is by making a hole in the floor of the cabin not high enough for the person to stand up in, with a crib over it to prevent his getting up, the hole is about five feet deep, and they give the wretched being his food there, and there he generally dies. Of all human calamity, I know of none equal to this, in the country parts of Ireland which I am acquainted with.’
Reports such as this resulted in the establishment of a vast network of public asylums across Ireland during the 1800s, based on the idea that, in the words of the Lunatic Asylums (Ireland) Commission (1858), ‘it is of the utmost importance that cases of insanity should as speedily as possible be removed to an asylum’. That is precisely what happened.
The Dangerous Lunatic Act (1838)
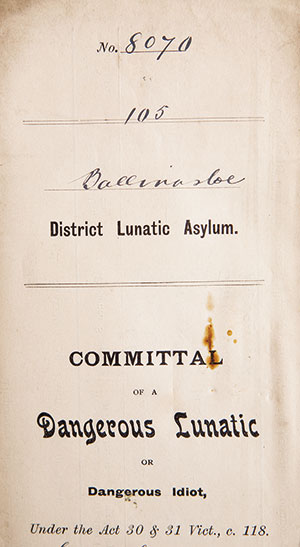
Above: A committal form under the Dangerous Lunatic Act (1838), which was widely misused, contributing to the rapid expansion of Ireland’s asylum system.
During the committal process, medical evidence could be heard (and generally was) but was not mandatory; certificates were signed by two magistrates. The 1838 Act soon became the admission pathway of choice for families seeking institutional care for relatives, and a habit grew of encouraging the mentally ill to commit minor offences to facilitate committal.
Many other factors also contributed to the growth of the Irish asylums: the Great Famine, poverty, philanthropic impulses, problems in workhouses, and changes in the structures of families, communities and Irish society throughout the 1800s. But if there was one single, standout event that set Ireland on a course towards mass institutionalisation of the mentally ill it was the 1838 act. Asylum doctors, including Woods in Killarney and Garner in Clonmel, objected vociferously, to little avail. The legislation was ill conceived, poorly implemented and grossly unjust. Even after it was revised later in the 1800s, its echoes reverberated through the asylum system for much longer, setting the tone for the dominance of institutional care well into the twentieth century.
The asylums were effectively unstoppable: by 1900 approximately 21,000 people, 0.5% of the population of the 32 counties of Ireland, were accommodated in the district asylums, with a small number of the mentally ill still in workhouses. The asylums were overcrowded, unhygienic and profoundly anti-therapeutic. While there were similar trends in other countries, Ireland’s asylums grew more rapidly than those elsewhere, were proportionately much larger at their peak and were especially slow to decline. By the mid-1900s, Ireland had more asylum beds per head of population than any other country in the world.
Once the buildings existed, they were quickly filled. Even vast campuses such as St Brigid’s in Ballinasloe and St Ita’s in Portrane were immediately overcrowded and expanded rapidly. Diagnostic systems and new terminologies evolved alongside the institutions, and recognised illnesses included ‘mania’, ‘melancholia’, ‘dementia’ and—puzzlingly—‘insane ear’. The latter referred to haematoma auris, a swelling of the earlobe owing to a collection of blood. This was initially thought to be connected with specific forms of ‘insanity’, including late-stage syphilis, epilepsy and mania. It was, however, eventually linked with the use of physical restraint by asylum staff, and this seems a more likely explanation in the often-harsh setting of the Irish asylums.
The role of medical professionals
One version of the history of psychiatry which seeks to explain institutional expansionism places strong emphasis on the emergence of the psychiatric profession and its possible role in generating increased committal rates. This narrative is supported by the fact that the complex, evolving psychiatric classification system used by medical superintendents during the 1800s undoubtedly reflected, at least in part, their growing desire for specialisation and recognition. Links between doctors’ pay and asylum size in the late 1800s further underline the role of the new professionals in the growth of the asylums.
This argument is certainly supported to the extent that the emergence of clinical professionals, both medical and nursing, throughout the 1800s and 1900s was inevitably a factor in shaping psychiatric practice in Ireland, as it did elsewhere. There is, however, little evidence that the search for professional prestige was the main driver of increased admission rates in Ireland, or that it was unconnected with broader societal concerns driving up committals.
In the first instance, the medical and nursing professions were by no means the only or even the main stakeholders in the Irish asylums. In 1951 the town of Ballinasloe had a population of 5,596, of whom no fewer than 2,078 were patients in the mental hospital. As a result, virtually everyone in the area was a stakeholder in the hospital in one way or another, and there is growing evidence that communities and families were powerful users and shapers of the system, acting in complex and often subtle ways, according to community and family needs. Most committals were instigated by hard-pressed families rather than governmental agencies or doctors, and it was not uncommon for families to remove relatives from asylums to work in the summer months and then return them in the winter (‘wintering in’).
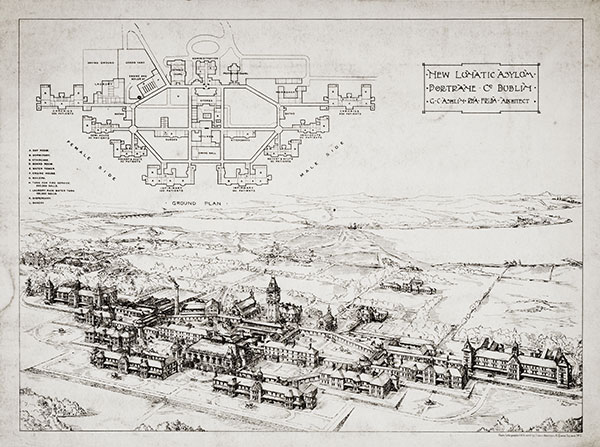
Above: The ‘new lunatic asylum, Portrane, Co. Dublin’, from the Building News and Engineering Journal, 27 April 1900. Despite their vast size, once such buildings existed they were immediately filled and soon overcrowded. (Irish Architectural Archive)
Indeed, for much of the nineteenth century medical opinion was not even required for committal, as many admissions were certified by justices of the peace, clergymen or others, and decided by hospital boards or courts. As a result, doctors were frequently obliged to admit, ‘treat’ and attempt to discharge people whom they did not believe to be mentally ill in the first instance. There is also evidence that asylum board members used their privileges to facilitate admissions from their own localities.
Most depressingly, perhaps, the archives of many asylums are replete with letters from asylum doctors urging families and governmental authorities to cooperate with the discharge of patients, often to little avail. Some families were simply too poor to receive home someone with enduring mental illness or intellectual disability, arguing that that person was better off in the asylum and should be kept there until he or she died.
The demise of the Irish asylum in the 1900s

Above: Dr James Foulis Duncan (1812–95), the last of the Duncan family to own Farnham House, a private asylum in Finglas, Co. Dublin. Duncan grew up there, and his earliest lessons in Latin, mathematics and science were provided by patients whom he later described as the best and noblest persons of the race. (Royal College of Physicians of Ireland)

Above: Dr Conolly Norman (1853–1908), a progressive-minded asylum doctor who served as resident medical superintendent of the Richmond Asylum, Grangegorman, from 1886 to 1908, and as president of the Medico-Psychological Association in 1894. (Royal College of Physicians of Ireland)
Against this distinctly dispiriting background, the early twentieth century saw a succession of novel biological treatments introduced in Irish mental hospitals out of a sense of therapeutic desperation if nothing else. These included malarial therapy (intentionally giving patients malaria to treat their mental disorder), insulin coma therapy (inducing fifteen-minute comas using insulin five days per week for several weeks), convulsive therapy (inducing seizures twice per week) and lobotomy (severing connections between different parts of the brain, permanently). Lobotomy was especially damaging, and insulin coma sometimes fatal. Electroconvulsive therapy remains in use today, but in a lesser, modified and highly regulated form.
Genuine reform, when it finally came in the mid-1900s, was attributable to improved legislation in the form of the (belated) Mental Treatment Act 1945, better treatments for mental illness (e.g. anti-psychotic medication) in the 1950s, the generally progressive Report of the Commission of Inquiry on Mental Illness in 1966, Ireland’s accession to the European Economic Community in 1973 and broader changes across Irish society during the 1970s, resulting in diminished tolerance for all kinds of institutions and increased concern about the fate of the mentally ill and intellectually disabled.
By 2015 there were under 2,400 patients in inpatient psychiatry beds, the vast majority of whom were voluntary patients admitted for short stays. Most people with mental illness are now treated outside of hospitals, in primary care or outpatient mental health services. While there remains much to be done to improve Ireland’s mental health services, the story has undeniably been one of considerable change over past decades. The shadow of the Irish asylum has not yet vanished completely but it has lessened substantially. Finally, perhaps, Conolly Norman would be pleased.
Left: Connaught District Lunatic Asylum (later St Brigid’s Hospital) was opened in Ballinasloe, Co. Galway, in 1833, at a cost of £27,000, with a capacity for 150 patients, but by 1951 it housed some 2,078 people. (Úna Spain/HSE).
Right: An empty corridor in St Brigid’s Hospital, Ballinsloe, today. Most people with mental illness are now treated outside of hospitals, in primary care or outpatient mental health services. (Úna Spain/HSE)
Brendan Kelly is Professor of Psychiatry at Trinity College, Dublin.
FURTHER READING
M. Finnane, Insanity and the insane in post-Famine Ireland (London, 1981).
B.D. Kelly, Hearing voices: the history of psychiatry in Ireland (Dublin, 2016).
J. Robins, Fools and mad: a history of the insane in Ireland (Dublin, 1986).
D. Walsh, ‘Mental illness in Ireland and its management’, in D. McCluskey (ed.), Health policy and practice in Ireland (Dublin, 2006).